Traitement chirurgical ; un traité sur les pratiques de traitement des maladies chirurgicales pour l'usage des praticiens et des étudiants de chirurgie . olicdownward. L'opération consiste à exposer l'artère mésentérique inférieure 592 TRAITEMENT CHIRURGICAL et la lier et la veine juste en dessous du lieu d'origine de l'artère colique gauche.le mésosigmoïde est ensuite divisé à partir du point de trompes à themiddle le sigmoïde de flexion. Les arches de la secondaire arteryshould sigmoïde pas être endommagé. Le péritoine est ensuite divisé le long de la innerside de l'artère à l'intérieur du mésorectum. L'lymphat
1345 x 1858 px | 22,8 x 31,5 cm | 9 x 12,4 inches | 150dpi
Informations supplémentaires:
Cette image appartient au domaine public, ce qui signifie que le droit d’auteur a expiré ou que le titulaire du droit d’auteur a renoncé à ses droits. Les frais facturés par Alamy couvrent l’accès à la copie haute résolution de l’image.
Cette image peut avoir des imperfections car il s’agit d’une image historique ou de reportage.
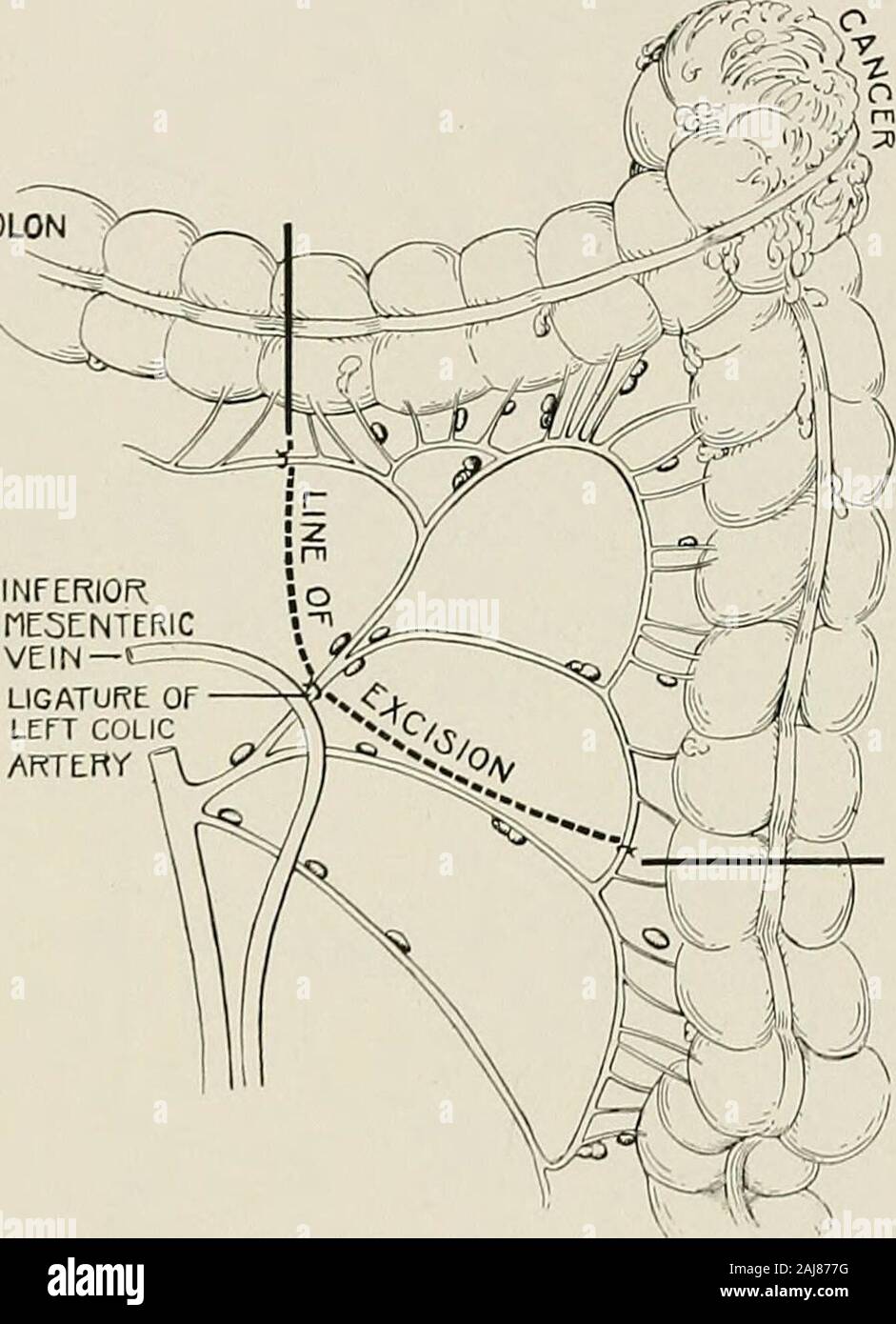
Surgical treatment; a practical treatise on the therapy of surgical diseases for the use of practitioners and students of surgery . olicdownward. The operation consists in exposing the inferior mesenteric artery 592 SURGICAL TREATMENT and tying it and the vein just below the place of origin of the left colic artery.The mesosigmoid is then divided downward from the point of ligation to themiddle of the sigmoid flexure. The secondary arches of the sigmoid arteryshould not be damaged. The peritoneum is then divided along the innerside of the artery to the inner side of the mesorectum. The lymphaticand mesocolic tissue is then stripped forward from the hollow of the sacrumand the middle sacral artery is tied. The peritoneal reflection between thebladder and rectum is then divided (Fig. 1243) (see Cancer of Rectum, Vol. III). For cancer of the middle and upper part of the sigmoid, the same procedureas described above is followed. A larger amount of mesocolon is removed.The bowel is divided above at the end of the descending colon, and below itshould be divided about 15 cm. (6 inches) beyond the growth (Fig. 1244). COLON. INFERIORI1E5ENTERICVEIN-LIGATURE OFLEFT COLICARTERY Fig. 1241.—Cancer of Splenic Flexure of Colon.Showing extent of colon and mesocolon to be removed. If the surgeon would take into account the lymphatics and eliminateevery possibility of recurrence, the operation must be carried out in compli-ance with these requirements. This is not possible in some cases, andnot necessary in others. Remarks on Cancer of the Colon.—Before operating everything shouldhave been done to put the patient in the best possible state of physicalresistance. A laxative should not be given within twenty-four hours of theoperation; if one is required it is best that it should be administered notnearer than forty-eight hours to the operation. The reason for this is thatif resection is done, it is better performed in the presence of a dry intestine withsolid contents than in the p
{kind=link}